
Cricothyroidotomy
Introduction
“Can’t intubate, can’t ventilate” (CICV) is a rare but potentially catastrophic scenario which may be encountered during intubation (Human Factors).
In the setting of a CICV emergency a range of front of neck access techniques are available. These can broadly be classified into needle based and scalpel based techniques. Due to limited evidence of technique success and a plethora of potential complications these techniques are reserved as an absolute last resort. However, when indicated they should be carried out expediently as they have the potential to be life saving. These techniques are relatively straightforward and the most challenging aspect is making the decision to perform them.
Current Guidelines
Current Difficult Airway Society (DAS) Paediatric guidelines suggests that in the setting of a CICV emergency then efforts should be taken to optimize oxygenation and ventilation with use of 100% oxygen, optimal airway positioning (Airway Anatomy), two person bag mask technique and oropharyngeal or supraglottic airway devices (LMA insertion). Reversal of intubation drugs should be considered if oxygenation is adequate (>80%) (Intubation Pharmacology).

Cannot intubate and cannot ventilate (CICV) in a paralysed and anaesthetised child aged 1 to 8 years. Paediatric difficult airway guidelines. Association of Paediatric Anaesthetists of Great Britain and Ireland/Difficult Airway Society, 2015. Reproduced with kind permission of APAGBI/DAS.
If this is unsuccessful then front of neck access should be considered. A skilled ENT surgeon should ideally perform this but, if unavailable, then the most appropriately skilled within the local team should attempt. DAS guidelines suggest that in those < 8 years of age needle cricothyroidotomy is first line with scalpel techniques reserved for situations where these techniques fail. Whilst in those > 8 years of age a scalpel technique is advocated for all front of neck access.
Current Advanced Paediatric Life Support (APLS) guidance suggests that needle techniques should only be attempted in children over the age of 5 years with scalpel techniques preferred in those <5 years (via tracheostomy in < 1 year and cricothyroidotomy or tracheostomy in 1-5 year olds).
Given this conflicting advice it would be ideal if a local institutional approach were developed to guide practitioners working within areas where a CICV scenario may arise. However, given the rarity of this scenario this is unlikely in most institutions.
As such it is the author’s belief that each reader should review the following techniques with a view to reaching a personal conclusion regarding which technique they would feel best equipped within their workplace to carry out should the need arise.
Needle Cricothyroidotomy
Needle cricothyroidotomy is a simple, potentially life-saving procedure. Trans-tracheal oxygen insufflation via needle cricothyroidotomy will allow patient oxygenation but not ventilation. Whilst potentially life saving, it is not a definitive airway, and will at best buy minutes prior to insertion of a Seldinger or scalpel airway. Thus, whilst siting a needle cricothyroidotomy contact should be made with local practitioners skilled in definitive airway placement (eg ENT / Anaesthetics).
Setup
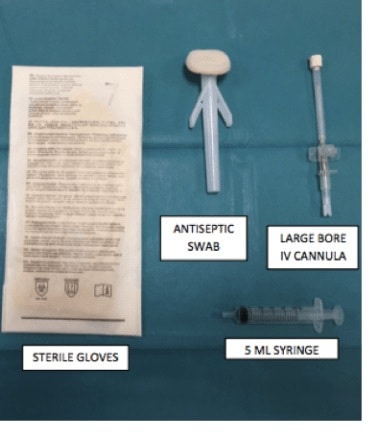
Suggested Cannula Size
Infants and children – 18G IV Cannula
Adolescent/Adult – 16G IV Cannula
Procedure
- Ensure definitive airway practitioners are requested to attend urgently.
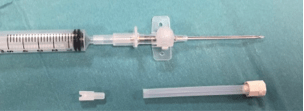
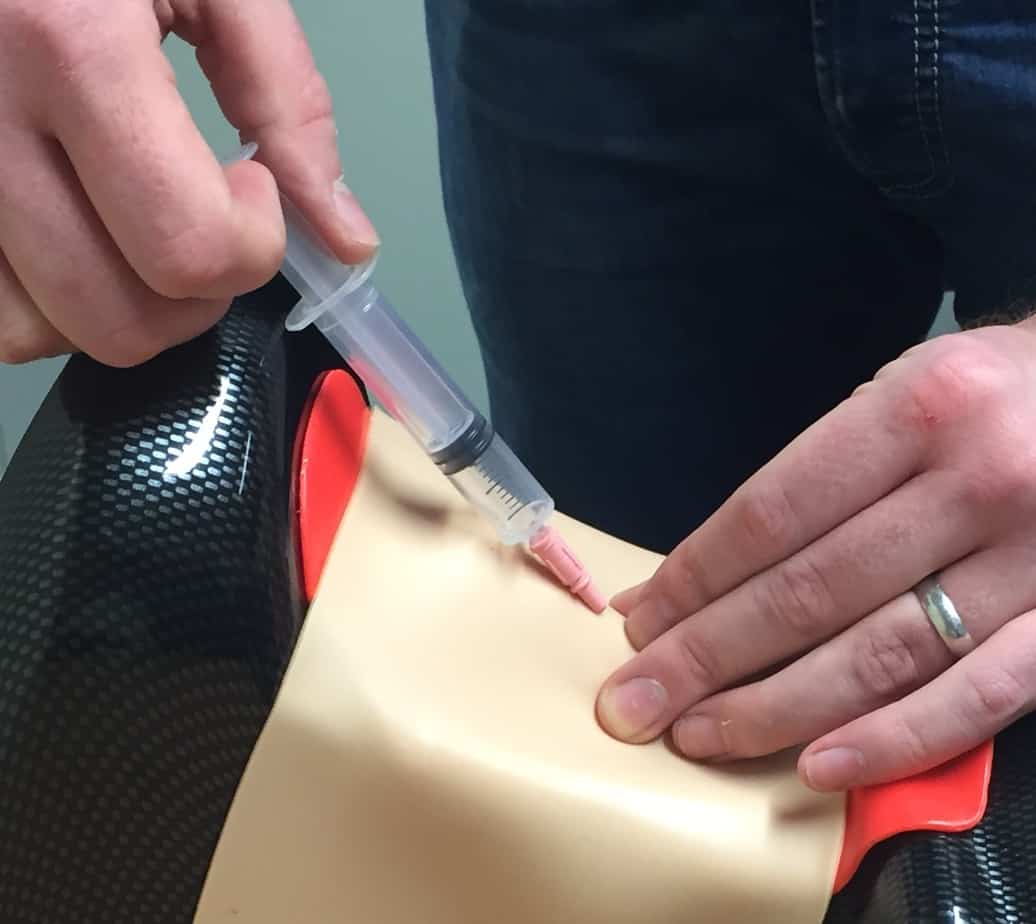
- Attach 5 ml syringe to cannula over needle.
- Identify cricothyroid membrane by palpation.

- If immediately available prepare the neck with antiseptic swabs.
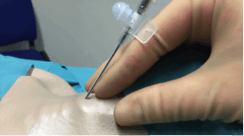
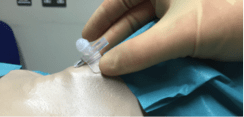
- Using your left hand stabilise the cricothyroid membrane.
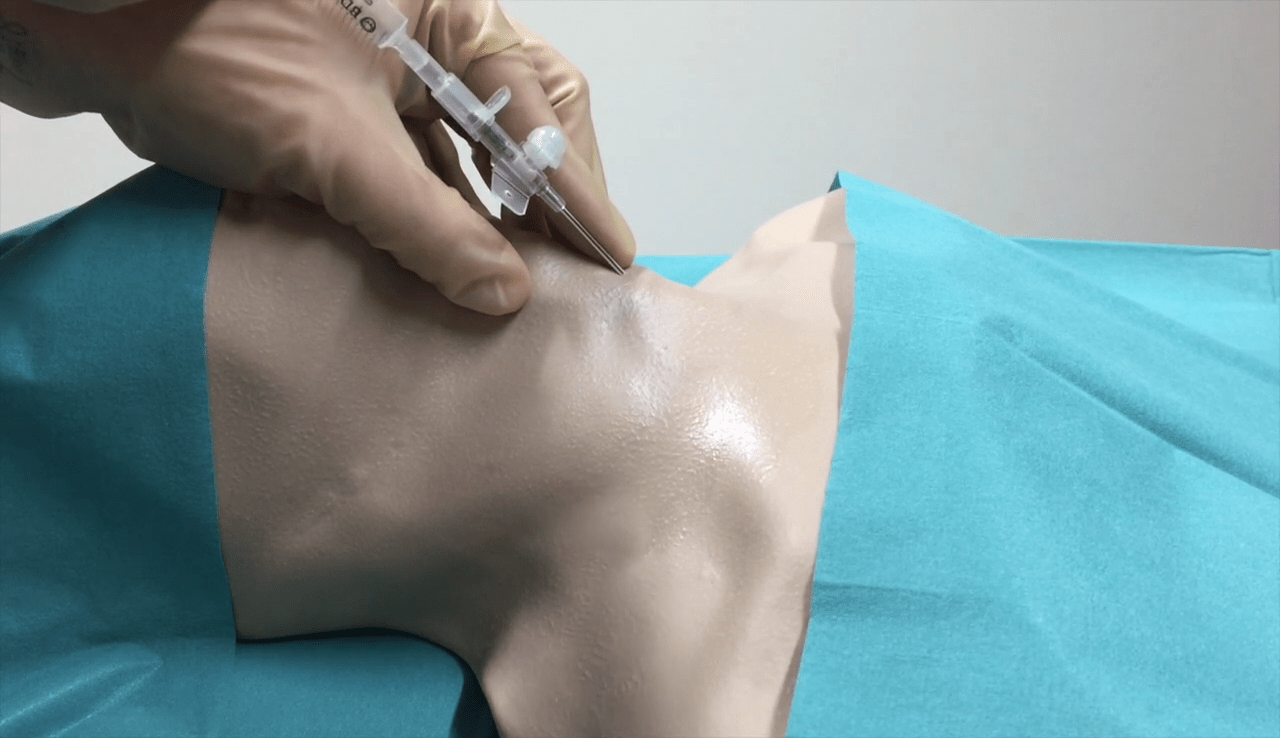
- Insert the needle and cannula through the cricothyroid membrane at 45 degrees caudally. Aspirate as you advance.
- Once air is aspirated carefully feed the cannula over the needle.
- Withdraw the needle.
- Attach commercially available cricothyroidotomy insufflation device to end of cannula and follow manufacturer instructions to provide oxygenation.
Useful Videos
Cannula Insertion. Reproduced with kind permission of Dr Andrew Heard MBChB, FRCA and the Anaesthetic Department at Royal Perth Hospital, Australia.
Jet Oxygenation. Reproduced with kind permission of Dr Andrew Heard MBChB, FRCA and the Anaesthetic Department at Royal Perth Hospital, Australia.
Seldinger Cricothyroidotomy
Following successful needle cricothyroidotomy the airway should be converted to a definitive airway as soon as possible. Commercially available procedure sets exist to allow conversion to a definitive airway via the Seldinger technique. This moderately complex technique allows for establishment of an airway through which both oxygenation and ventilation are possible.
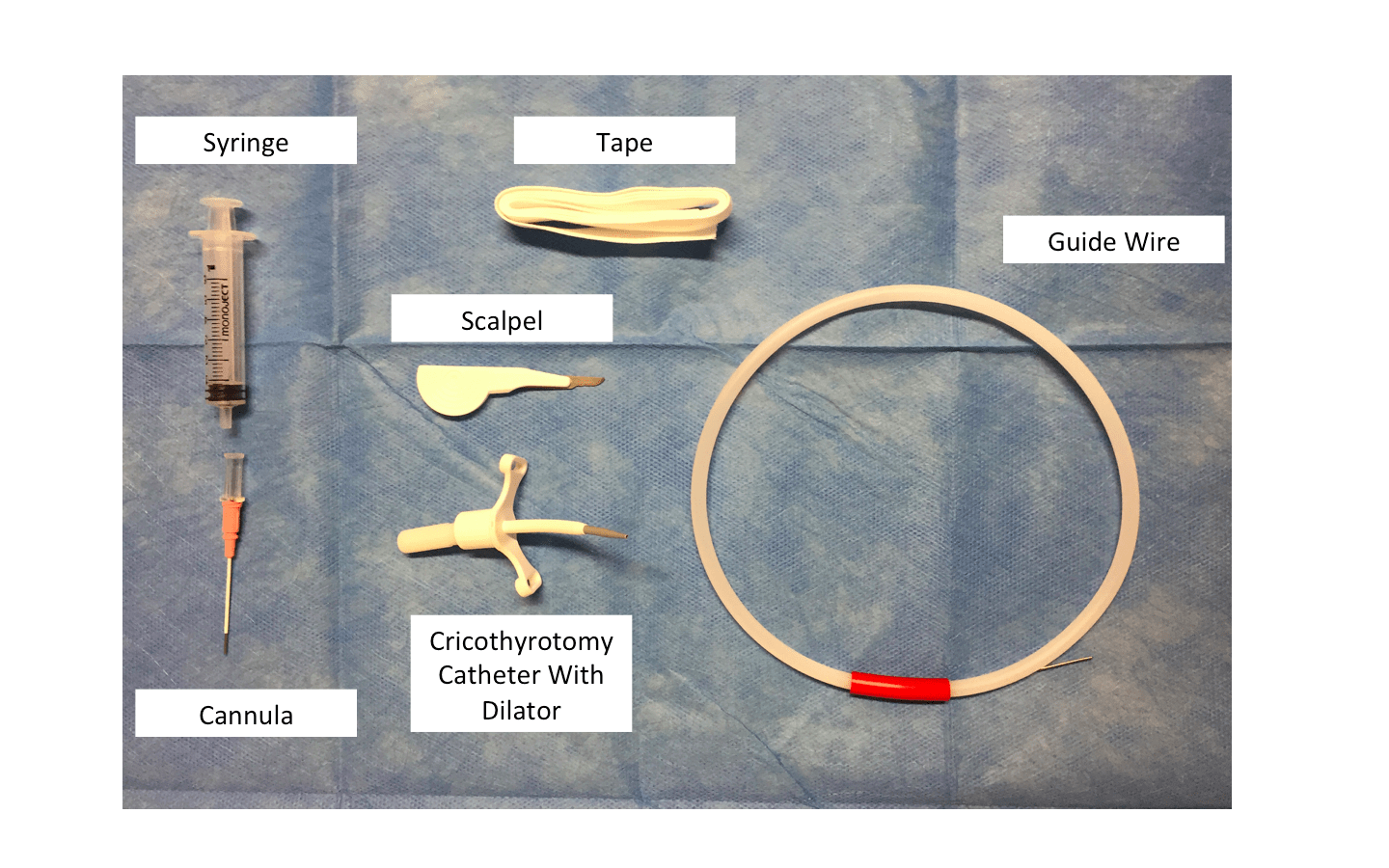
Setup
Procedure
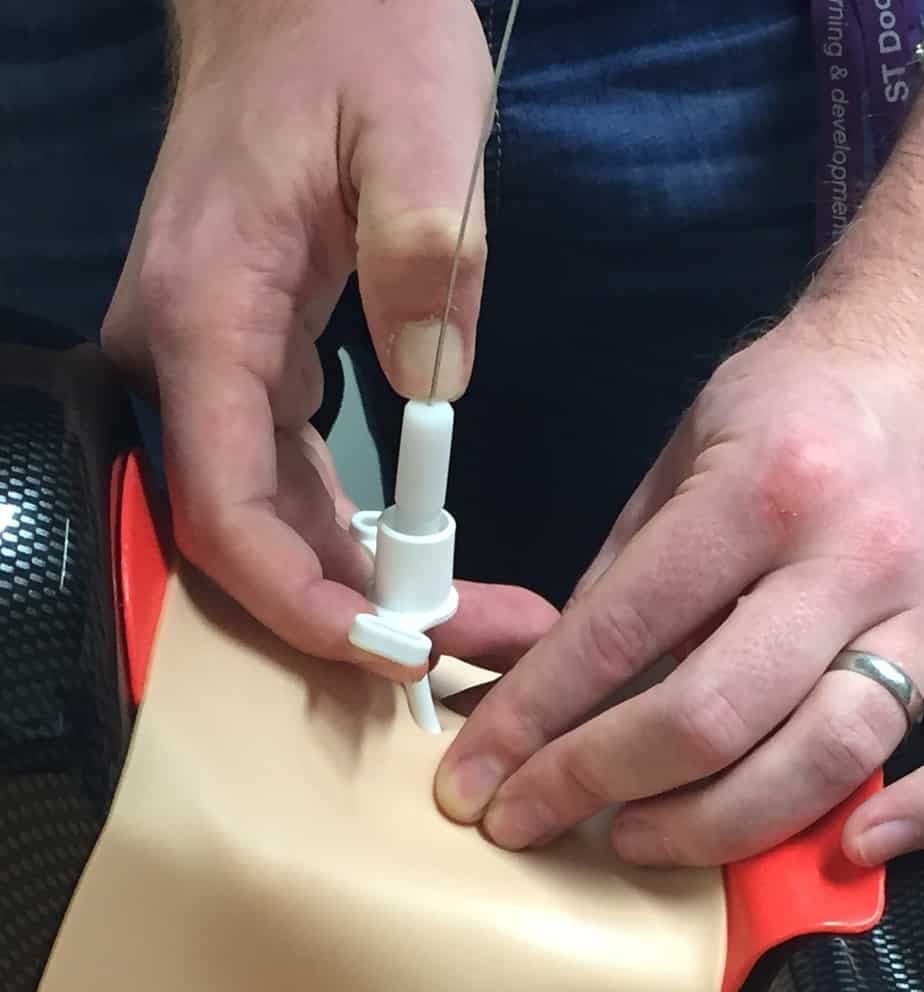
- Insert and confirm placement of a needle cricothyroidotomy cannula as detailed above.
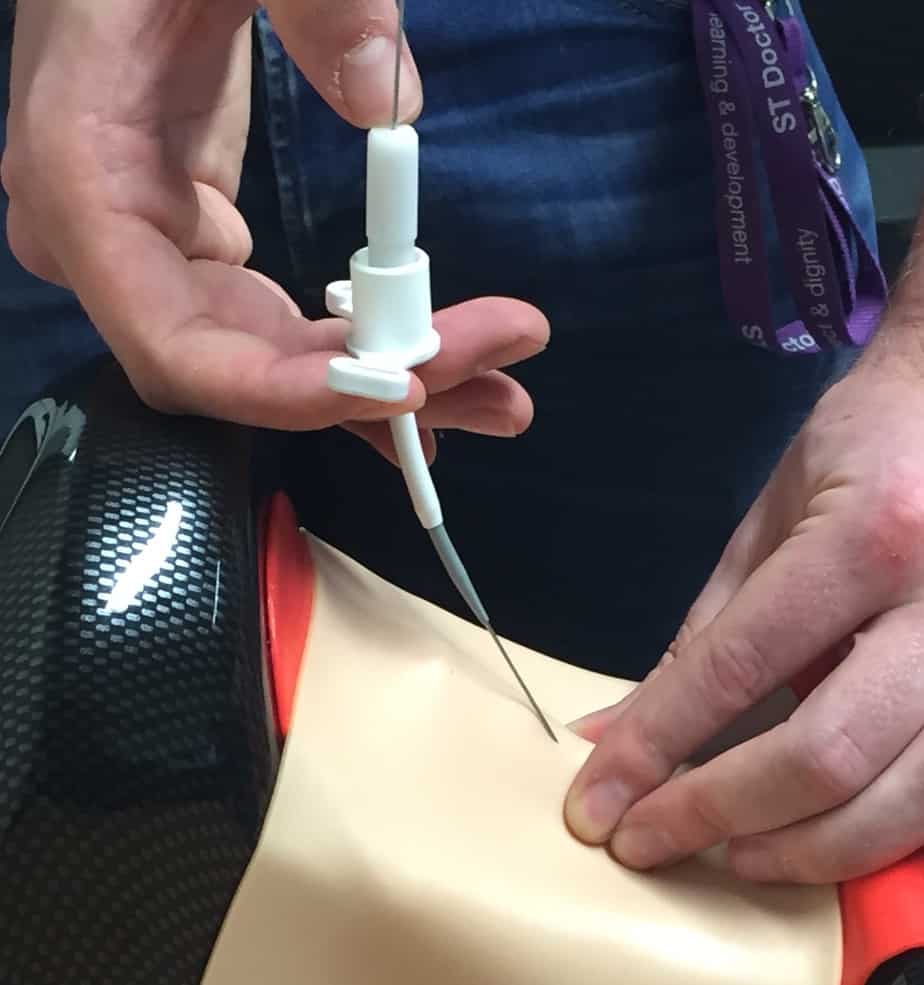
- Insert the guide wire through the cannula into the airway.

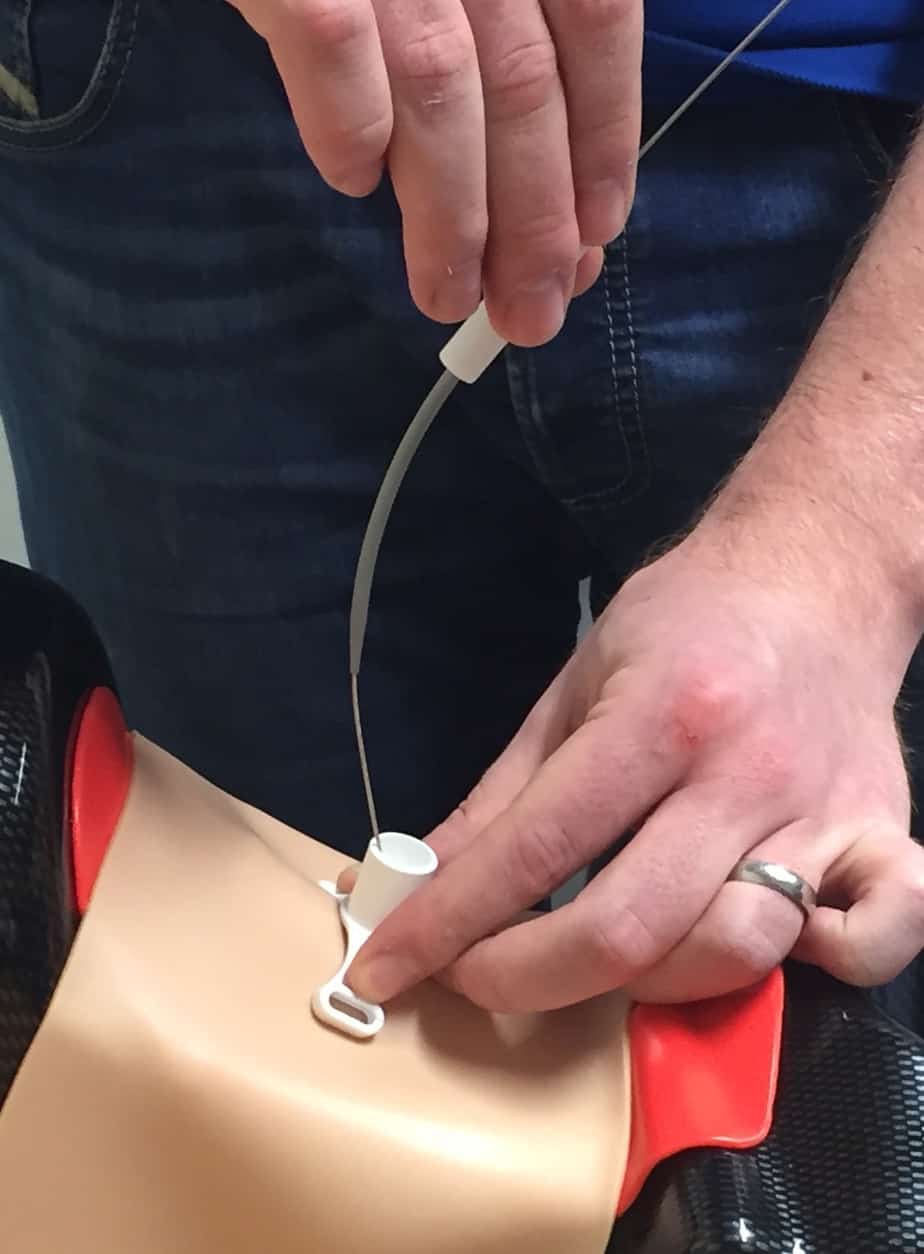
- Withdraw the cannula keeping the guide wire in place.

- Make a stab incision in line with the guide wire at the point where the wire pierces the skin.

- Feed the emergency cricothyrotomy cannula and dilator as one over the guidewire.
- Gently rotate the dilator and cricothyrotomy cannula and advance through the skin into the airway.
- Withdraw the dilator and guide wire leaving the cricothyrotomy cannula in place.
- Self inflating bags, anaesthetic bags or ventilators can now be attached to the cricothyrotomy cannula via universal connectors.

- The cricothyrotomy cannula should be secured in place with tracheal tape.
Useful Videos
Melker Insertion. Reproduced with kind permission of Dr Andrew Heard MBChB, FRCA and the Anaesthetic Department at Royal Perth Hospital, Australia.
Scalpel Bougie Cricothyroidotomy
During a CICV scenario where a needle technique fails then the scalpel bougie technique should be undertaken. This is the most invasive (and bloody) front of neck access technique. However, it is still relatively straightforward and when performed can establish a definitive airway.
Setup
Procedure
- If immediately available prepare the skin with aseptic swabs.
- Identify cricothyroid membrane by palpation.
- Make a horizontal stab incision with the scalpel, sharp edge toward yourself. A give is felt as the airway is entered.

- Rotate the scalpel so the sharp edge points caudally.
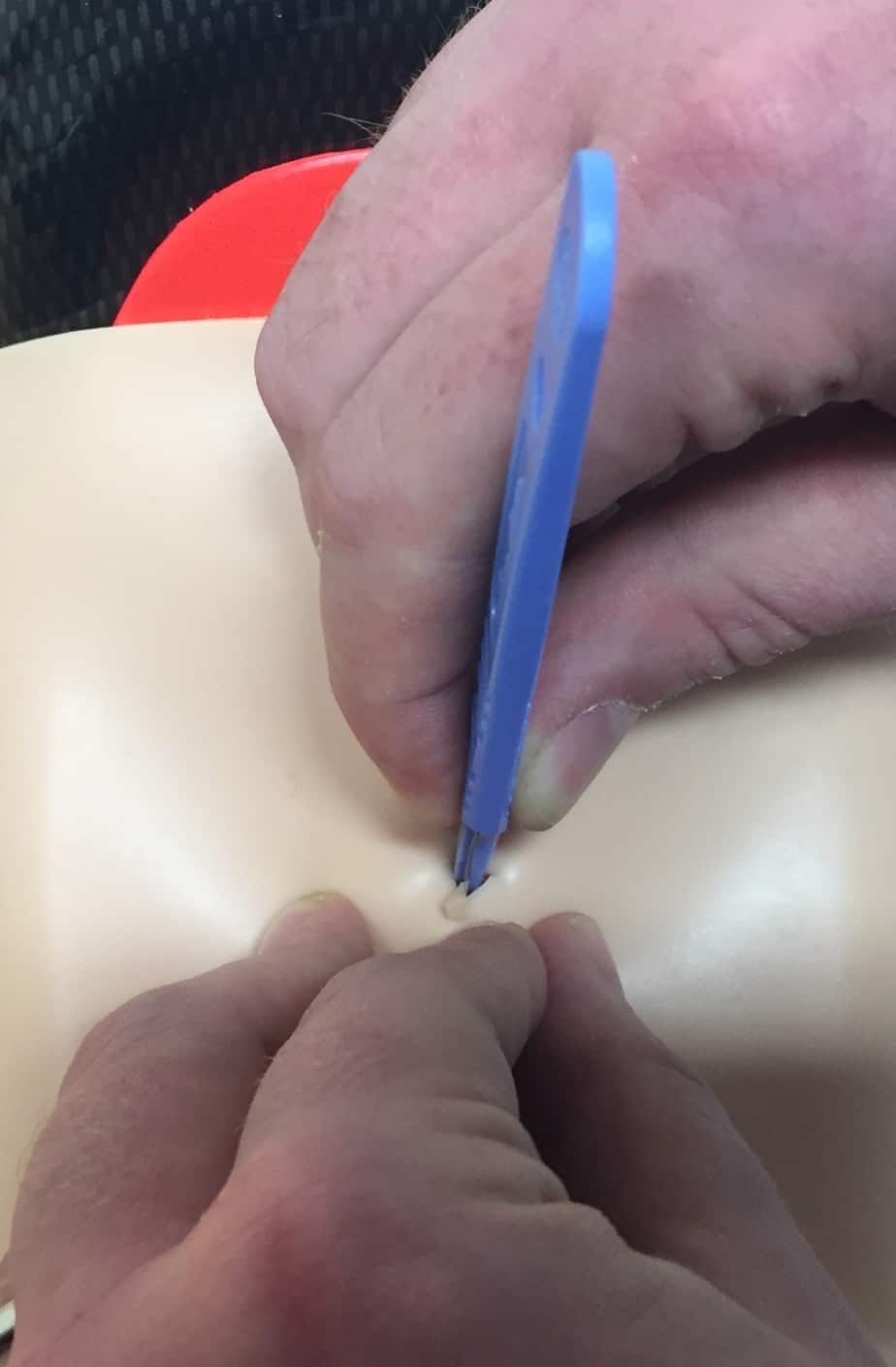
- Draw the scalpel toward yourself, keeping it perpendicular to the neck, and stabilise with your left hand. This should create a triangular opening in the skin into the airway.
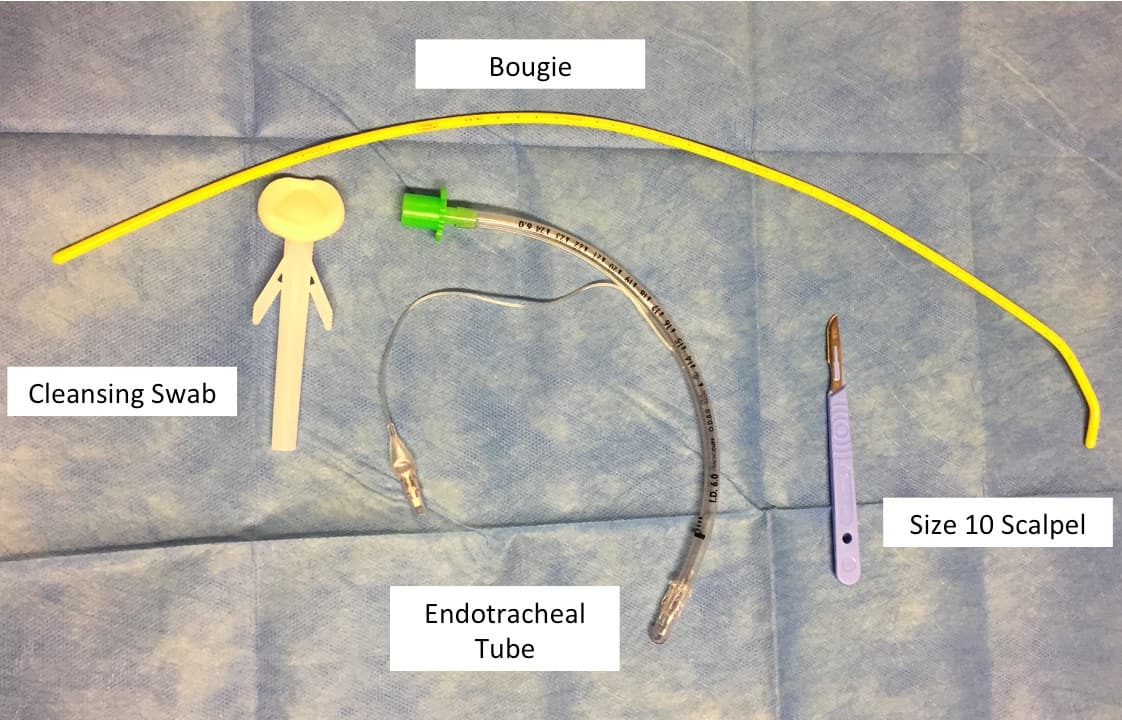
- Using the scalpel as a guide advance a bougie into the airway. Bougie size is determined by the size of ETT you wish to insert (airway anatomy and intubation preparation).
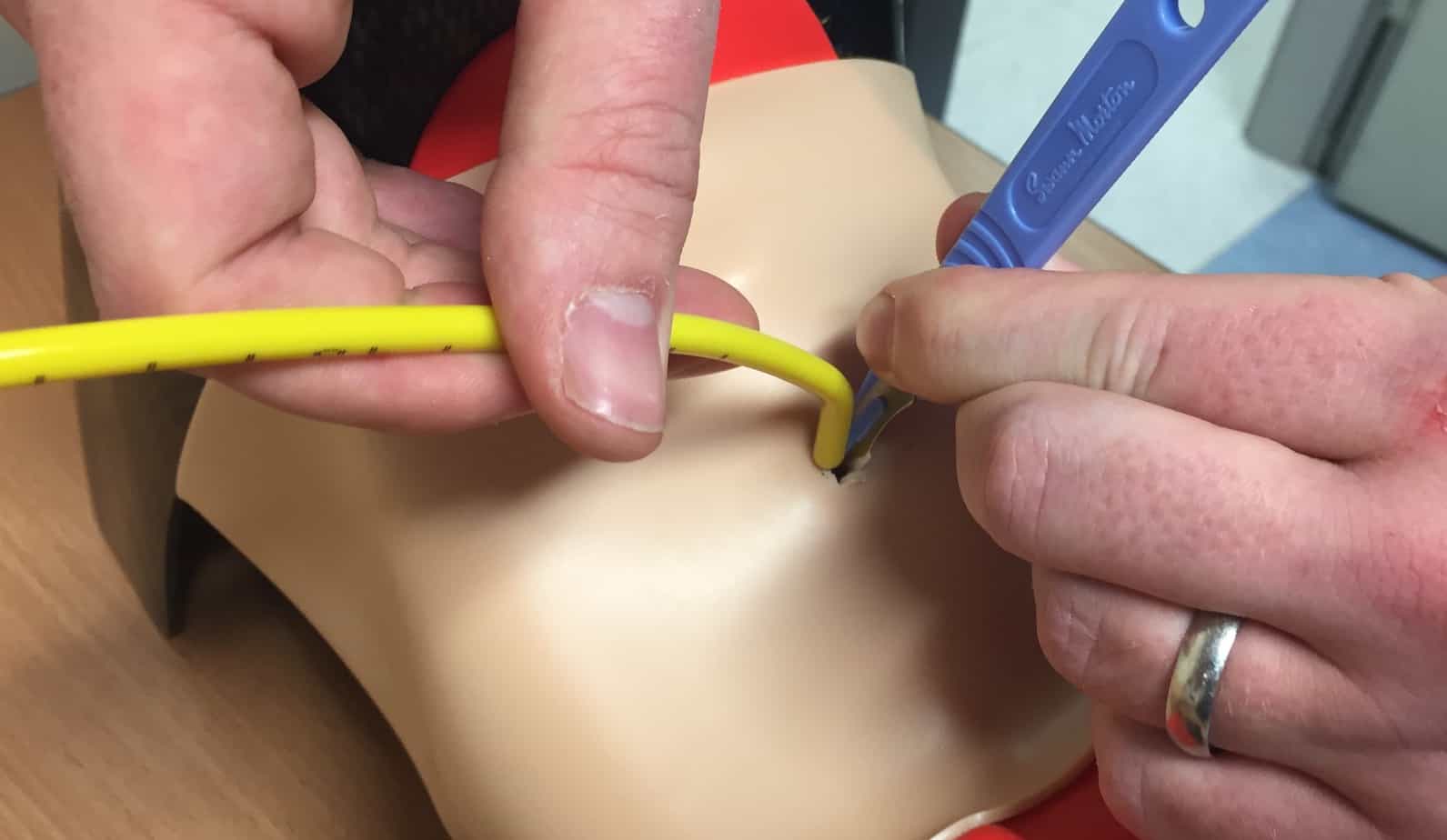
- Feed the bougie until the sensation of tracheal rings or hold-up is experienced.

- Feed an ETT or tracheostomy tube onto the bougie and advance through the skin using a rotating motion.

- Once in the airway inflate the ETT/tracheostomy cuff and withdraw the bougie.

- Self inflating bags, anaesthetic bags or ventilators can now be attached via universal connectors.
- The ETT / tracheostomy tube should now be secured in place.
Useful Videos
Scalpel Bougie. Reproduced with kind permission of Dr Andrew Heard MBChB, FRCA and the Anaesthetic Department at Royal Perth Hospital, Australia.
Conclusion
The CICV scenario is a rare but potentially catastrophic scenario, which may be encountered during intubation. A variety of relatively straightforward, potentially life saving, techniques are available to attempt to salvage the situation. These techniques should be considered an absolute last resort but should be carried out expediently where the need arises.
![]()