
Direct Laryngoscopy
Listen to Lecture
The process of direct laryngoscopy involves use of a laryngoscope to move the tongue and epiglottis out of the way allowing the laryngeal opening to be seen directly when looking through the patients mouth. It is vital that the patient is appropriately positioned prior to starting (see Intubation Preparation and Equipment) so that the oral, pharyngeal and tracheal axes are brought into alignment.
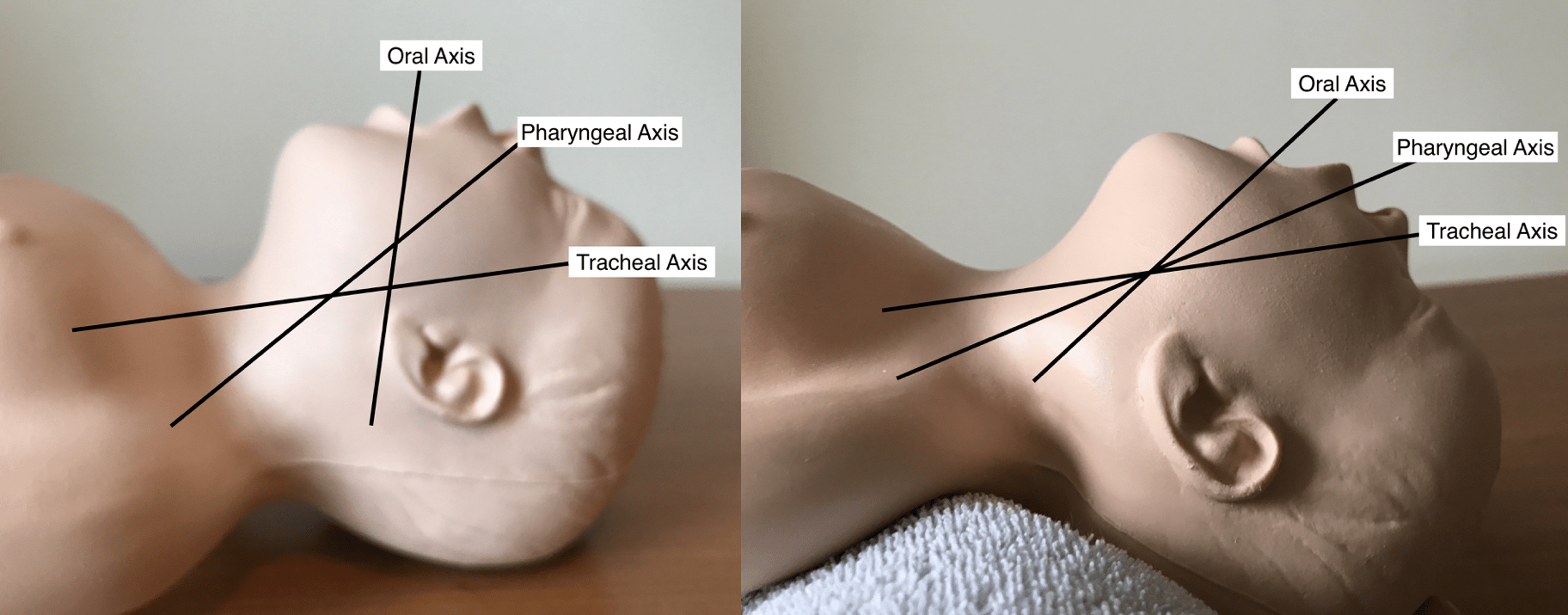
Alignment of oral, pharyngeal and tracheal axes by using a shoulder roll in a neonate
Success with this technique relies on systematic step by step approach as outlined below.
Holding the laryngoscope

Holding the laryngoscope near the blade like a pen compared to standard grip used when intubating adults
The laryngoscope should always be held in your left hand regardless of your hand dominance. When intubating neonates and infants the laryngoscope is best held near the blade, with a grip similar to how you would hold a pen. This will give you move control over the laryngoscope tip which is useful when lifting the epiglottis directly with a straight blade, but still allows application of the minimal lifting force needed to expose the laryngeal opening. When intubating older children the laryngoscope should be held in a similar way to how it is used in adults, as this allows the additional lifting force required to expose the laryngeal opening to be easily applied.
Opening the mouth

Scissor opening the mouth of an older patient and opening the mouth by placing a finger on top of the tongue in a neonate
The mouth should be scissor opened by applying pressure with you right thumb on the lower incisors and you right index finger over the upper incisors. In neonates and infants simply placing your right index finger on top of the tongue is often all that is required and this also prevents the laryngoscope from being inserted under the tongue.
Inserting the laryngoscope
The laryngoscope should then be inserted into the mouth and down the right hand side of the tongue, taking care not to catch the lips during insertion. When using a curved blade occasionally it may be difficult to insert the laryngoscope into the mouth directly as the handle catches on the patients chest (more common if a long handle is used or in obese patients or those with limited neck movement). To avoid this problem the laryngoscope can be rotated into the mouth from the side.
Video demonstrating the technique for rotating the laryngoscope into the mouth
Tongue control

Tongue pushed all the way over to left hand side by laryngoscope blade
The laryngoscope is designed to be inserted down the right hand side of the tongue and to push the tongue towards the left hand side of the mouth. Failure to do this (going directly over the tongue) will make the laryngeal opening appear more anterior than it actually is and often results in a more difficult angle to pass the endotracheal tube.
Find the epiglottis

Epiglottis coming into view
You should advance the blade slowly down the pharynx searching of the epiglottis. This is the key landmark in orientating yourself in the patients airway. Once found, whether your can see the laryngeal opening or not, you know where it should be in relation to the epiglottis and can focus your attention here while further adjustments to expose the laryngeal opening are made.
Exposing the laryngeal opening
Once the epiglottis has been found either lift it directly using a straight blade or pass the tip of the curved blade into the vallecula and by applying pressure on the glossoepiglottic ligament expose the laryngeal opening. Regardless of which method you use it is important that the lifting pressure with the laryngoscope is applied by pulling the laryngoscope away from yourself (aim for where the wall facing you meets the ceiling) rather than rocking or levering the laryngoscope handle backwards (risks damaging the patients lips, gums or teeth and often results in an inferior view).

Correct angle for applying lifting force with laryngoscope
Occasionally when using a straight blade you may find it difficult to lift the epiglottis directly and in this situation you have two options. Firstly, you can insert the laryngoscope too deep so that a view of the oesophagus is obtained, then gradually withdraw the laryngoscope till the laryngeal opening drops into view. Take care not to stop withdrawal at this stage as withdrawing further will cause the epiglottis to fall down again and block the view. The second option is to use the straight blade like a curved blade by inserting it into the vallecula. Be aware that using this technique in small infants will often result in a worse view than if the epiglottis was lifted directly, as laxity of the glossoepiglottic ligament and large floppy epiglottis in this age group often results in an incomplete laryngeal exposure (the reason you elected to use a straight blade in the first place). However when combined with bimanual laryngoscopy (external manipulation of the larynx by the intubator) a satisfactory view allowing intubation is obtained most of the time.
Optimise the view

External laryngeal manipulation applied using little finger of left hand in neonate or right hand in older patient
Unless you have a Cormack-Lehane grade 1 view you should attempt to improve the view by using external laryngeal manipulation. This should initially be bimanual where the intubator uses their right hand to apply pressure to the larynx externally and moves it about to find the position that gives the best view of the laryngeal opening. Once this has been found the larynx should be held in this position by the airway assistant, freeing up the intubator’s right hand to pass the tube. Alternatively in infants this can be done yourself by using the small finger on your left hand to maintain external laryngeal manipulation.

Additional room for passage of the endotracheal tube has been created by moving laryngoscope blade all the way to the left hand side of the mouth
To increase the room available to pass the tube ensure the laryngoscope blade is positioned well over towards the left hand side of the mouth, leaving lots of space at its right hand side.
Inserting the endotracheal tube

Correct technique for passing the endotracheal tube from the corner of the mouth
The endotracheal tube should be passed from the right hand side of the mouth, rather than straight down as this helps prevent the endotracheal tube from blocking the view of the laryngeal opening as it is passed. The angle for insertion can be improved by having the airway assistant apply lateral pressure to the cheek at the right corner of the mouth.

Pulling the corner of the mouth to improve the angle for insertion of the endotracheal tube
It is not uncommon that the endotracheal tube passes through the cords, but then its tip becomes stuck on the anterior tracheal rings preventing further passage down the trachea. This is more common in older children due to their well developed tracheal rings and with nasal intubation due to the angle of insertion (the trachea runs in a slightly posterior direction away from the larynx and the nasal tube starts in a posterior position and is directed anteriorly towards the laryngeal opening). If this happens the endotracheal tube should be withdrawn slightly (removing it from the tracheal ring it has become caught on) and then by rotating the tube anticlockwise while advancing it, the bevel on the endotracheal tube tip should roll of the tracheal ring, allowing the tube to be advanced into the trachea. With nasal intubation it can be difficult to achieve enough rotation of the tube to overcome this problem and it is often more effective to use forceps to direct the tip of the tube more posteriorly (matching the angle of the trachea).
Nasal Endotracheal Intubation
A nasal endotracheal tube is generally regarded as being more comfortable for the child and is more secure, with a lower risk of unplanned extubation. However nasal intubation is technically more difficult than oral intubation and even in experienced hands takes slightly longer and there is no way to tell how the critically ill child will tolerate this delay. Also nasal intubation is contraindicated in patients who may have a basal skull fracture or who are at increased risk of bleeding e.g. deranged clotting or thrombocytopenia (which may not be known about at presentation).
With this in mind the critically ill child should be intubated orally initially as this is the fastest way to secure the airway and also the route most likely to succeed. The endotracheal tube can then be converted to a nasal tube provided the child is stable, it is not contraindicated and the benefits of doing so outweigh any risks. It must be remembered that the best endotracheal tube is the one that is in the trachea and the practise of converting a functioning oral endotracheal tube to a nasal tube, just because of local preference, in an unstable patient e.g. septic shock or post arrest patient, is both unnecessary and dangerous and must be strongly discouraged.
Oral to nasal endotracheal tube conversion
Video demonstrating the technique for oral to nasal endotracheal tube conversion
- Loosen any tapes securing the oral endotracheal tube and move it from the right-hand side to the left-hand side of the mouth.
- Have an assistant hold it there and continue to ventilate the patient via the oral endotracheal tube throughout the procedure (ensure that they hold the tube from the side and that their hand and tubing are away from below the patients mouth where it can get in the way of the laryngoscope.
- Pass a second lubricated endotracheal tube down the patients nostril, stopping once a give is felt as the tube enters the pharynx. If there is any difficult advancing the tube try the other nostril or consider passing over a suction catheter.

Suction catheter inserted in endotracheal tube to help passage down nose
- Insert laryngoscope and obtain a view of the laryngeal opening using the steps described above.
- Suction around laryngeal opening and pharynx (nasal tube often sits in a pool of secretions in posterior pharynx)
- If necessary adjust the length that you have inserted the nasal tube to so that it’s tip is positioned midway between the end of the soft palate and laryngeal opening (manipulate tube at nose). If tip of nasal tube is not visible push oral tube to left with forceps as this often hides the nasal tube (more common if inserted in left nostril).
- Grab nasal tube tip with forceps and position at laryngeal opening so that you could pass the nasal tube if oral tube was not there.
- You won’t be able to see the laryngeal opening with the oral tube in situ, but you should identify the posterior laryngeal cartilages below the oral tube to ensure you have an adequate view.

Posterior cartilages (arrowed) visible below endotracheal tube indicating adequate view with oral endotracheal tube in situ
- Once happy ask the assistant to withdraw the oral tube and pass nasal tube. If tube won’t pass with forceps either leave at laryngeal opening and push tube at nose or rotate tip posteriorly using forceps. Ensure you leave enough time to replace oral tube if nasal tube won’t pass.
- Check depth marker position prior to removal of laryngoscope, making any adjustments to length at the nose.
![]()