

Listen to the Podcast
Push Dose Pressors

Normally vasoactive drugs are given in concentrated infusions via a central line. In contrast ‘Push Dose Pressors’ are titrated by administering small aliquots from a dilute vasoactive drug syringe by bolus injection, normally via a peripheral line. Due to the speed at which they can be initiated ‘Push Dose Pressors’ are used primarily in the crashing peri-arrest patient to obtain stability, where starting a standard infusion of the drug would take too long (they buy time while a standard vasoactive drug infusion is prepared and started) or where the duration of hypotension is expected to be short lived, making a standard infusion unnecessary e.g. hypotension following induction of anaesthesia. There are a number of drugs that are commonly used as ‘Push Dose Pressors’ but as adrenaline is one of the most effective, best suited to the crashing child and is easily available on every resuscitation trolley in the hospital, it is the one I would recommend using.
Instructions for Preparing Push Dose Adrenaline

Peripheral Adrenaline Infusion
There is a common misconception that vasoactive drugs must only be given via a central line. There is increasing evidence that peripheral vasoactive drugs are safe to use in an emergency situation prior to insertion of a central line (they are certainly more safe than withholding a lifesaving drug from your patient, just because you don’t have the gold standard access). Like with ‘Push Dose Pressors’ there are a number of different drugs that can be administered in dilute continuous infusions in an emergency, but for the same reasons mentioned above adrenaline is the one I would recommend using.
Instructions for Preparing a Peripheral Adrenaline Infusion

Key Learning Point

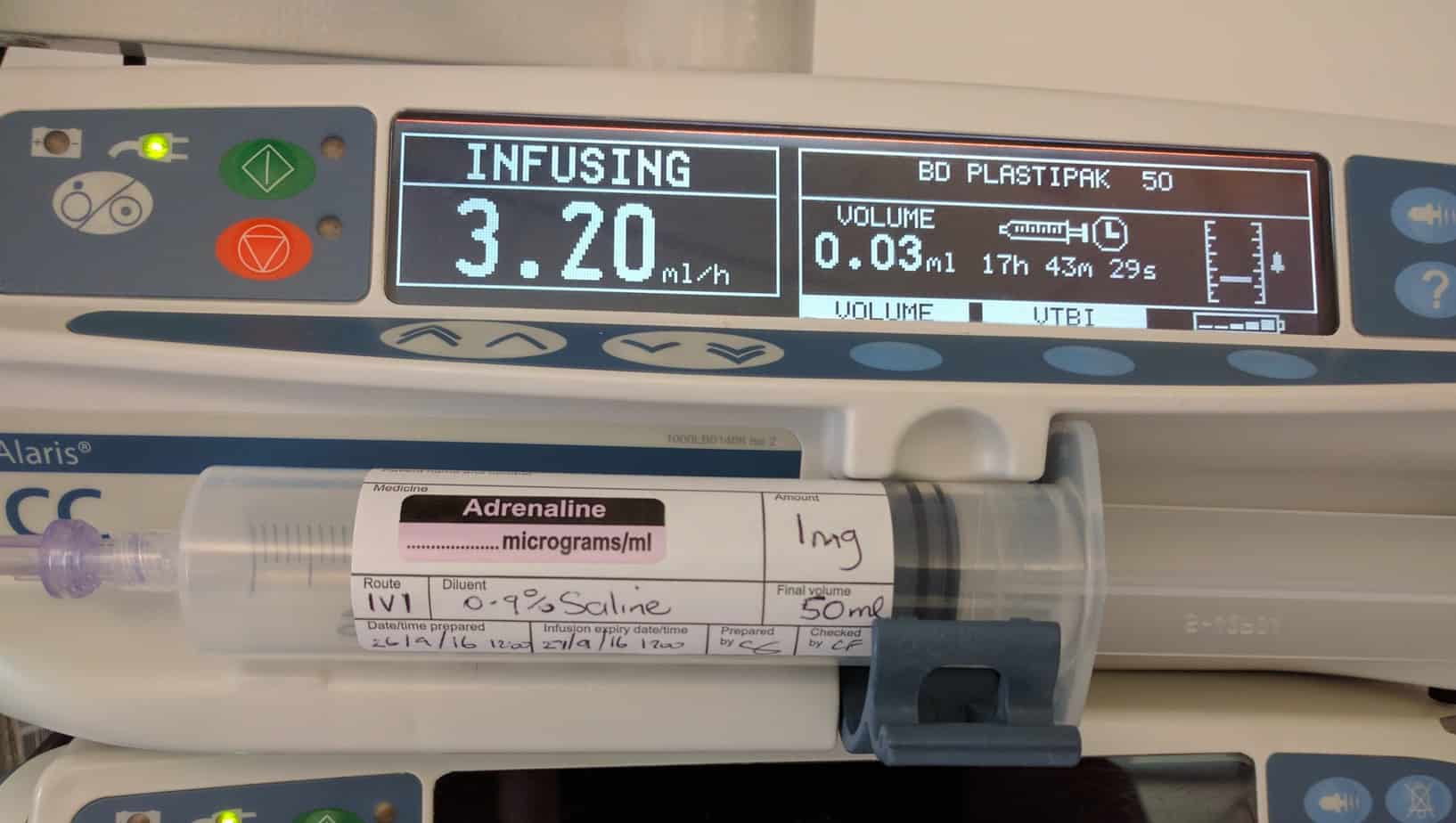
It is vital that you know the dead space of any line/extension set you use and factor this in when starting important infusions such as adrenaline. For example the pictured cannula has a dead space of 0.1 ml and the extension set of 0.3 ml, therefore if standard strength peripheral adrenaline infusion (1 mg in 50 ml of 0.9% saline) is started in a 3 kg baby at the normal starting dose of 0.1 mcg/kg/min it will take 27 minutes for the drug to reach the patient through the dead space. If the dead space is known this volume can be safely bolused, allowing for immediate delivery of a lifesaving drug.
Which Should I use?
For the shocked hypotensive patient I generally prefer to start a peripheral adrenaline infusion in preference to ‘Push Dose Pressors’ if time allows as it tends to cause less swings in blood pressure and can be administer by a pump rather than a member of the team, who can then be freed up to carry out another task. If the child needs adrenaline immediately I will start with push dose pressors and convert to a peripheral infusion at a later stage.
![]()
Very excellent material.
Thanks for your time spend to help to save children lives.
Keep it up Chris
Thanks Mohamed, hope the new job is going well. Keep in contact. Chris
Fantastic podcast, thanks a lot for taking the time to produce them
Glad you found it useful
Excellent stuff
What article or evidence is there behind the dose used for push adrenaline to maximize pre load prior to a drip
Good practical advice Chris. I’ll use it tomorrow on the Telelink.
Hi Chris,
I have a suggestion to make it simple to calculate push-dose adr and would love to know your thoughts.
Take the child’s 10mcg/kg resus dose, make this up to 10mls with 0.9% NaCl, then give in 1ml aliquots which is 1mcg/kg.
The 10mcg/kg resus dose is often given on paeds drug calculators for ease.
E.g.
Step 1 – 12kg child, 10mcg/kg = 120mcg = 1.2ml of 1:10,000
Step 2 – make this to 10mls giving 10mcg/kg in 10 mls = 120 mcg in 10 mls
Step 3 – give this in 1ml aliquots = 1mcg/kg dose = 12 mcg in 1 ml in this case